コロナワクチン接種後の合併症

タクヤ@自己免疫漢方治療専門の毛髪診断士
海外では特にワクチン接種後による小児の多系統炎症症候群が報告されています。
以前よりも小児のワクチン接種率が上がったのが原因だと思います。
「世界一わかりやすいワクチン後遺症」でも書きましたが、今回のワクチンは「コロナウィルスの種」を「体内で育てるワクチン」です。
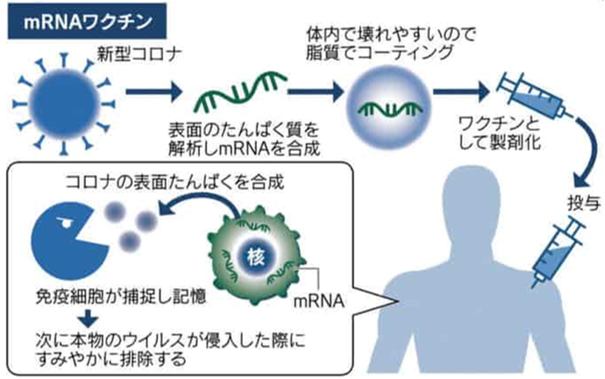
新型コロナウイルスの抗原に対する宿主の過剰な免疫応答が原因とすると、それが本物のウイルスでも、mRNAワクチンによって体内で作られた抗原でも良いわけなので、このような疾患群も十分ありえます。
成人でも報告されています。
ワクチン接種後に起きる多系統炎症症候群は川崎病を疑わせるような多臓器に強い炎症を起こす病気です。
症状は、発熱、腹痛、下痢、全身臓器の障害、特に心機能の低下がみられるのが特徴です。発疹、結膜炎、粘膜病変を生じることもあるところが、川崎病と似ています。
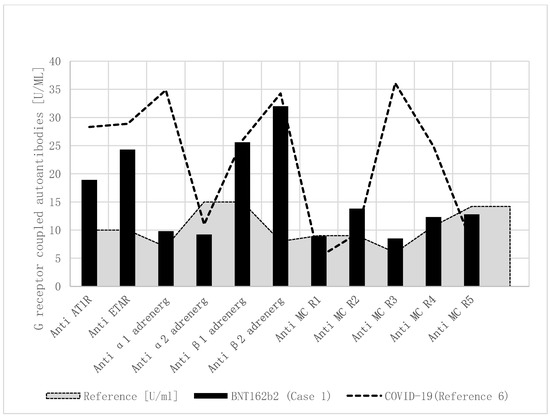
Autoantibody Release in Children after Corona Virus mRNA Vaccination: A Risk Factor of Multisystem Inflammatory Syndrome?
Multisystem inflammatory syndrome (MIS) is a new systemic inflammatory acute onset disease that mainly affects children (MIS-C) and, at a lesser frequency, adults (MIS-A); it typically occurs 3–6 weeks after acute SARS-CoV infection. It has been postulated and shown in adults that MIS may occur after SARS-CoV-2 vaccination (MIS-V). Our current case is one of the first published cases with a multisystem inflammatory syndrome in an 18-year-old adolescent after the SARS-CoV-2 vaccine from Pfizer/BionTech (BNT162b2), who fulfills the published level 1 criteria for a definitive disease: age < 21 years, fever > 3 consecutive days, pericardial effusion, elevated CRP/NT-BNP/Troponin T/D-dimeres, cardiac involvement, and positive SARS-CoV-2 antibodies. The disease starts 10 weeks after the second vaccination, with a fever (up to 40 °C) and was treated with amoxicillin for suspected pneumonia. The SARS CoV-2-PCR and several antigen tests were negative. With an ongoing fever, he was hospitalized 14 days later. A pericardial effusion (10 mm) was diagnosed by echocardiography. The C-reactive protein (174 mg/L), NT-BNP (280 pg/mL), and Troponin T (28 pg/mL) values were elevated. Due to highly elevated D-dimeres (>35,000 μg/L), a pulmonary embolism was excluded by thoracal computer tomography. If the boy did not improve with intravenous antibiotics, he was treated with intravenous immunoglobulins; however, the therapy was discontinued after 230 mg/kg if he developed high fever and hypotension. A further specialized clinic treated him with colchicine and ibuprofen. The MIS-V was discovered late, 4 months after the onset of the disease. As recently shown in four children with MIS-C after SARS-CoV-2 infection and a girl with Hashimoto thyroiditis after BNT162b2 vaccination, we found elevated functional autoantibodies against G-protein-coupled receptors that may be important for pathophysiology but are not conclusive for the diagnosis of MIS-C. Conclusion: We are aware that a misattribution of MIS-V as a severe complication of coronavirus vaccination can lead to increased vaccine hesitancy and blunt the global COVID-19 vaccination drive. However, the pediatric population is at a higher risk for MIS-C and a very low risk for COVID-19 mortality. The publication of such cases is very important to make doctors aware of this complication of the vaccination, so that therapy with intravenous immunoglobulins can be initiated at an early stage.
小さいお子さんがコロナワクチンを接種するときは充分に主治医と相談してください。








